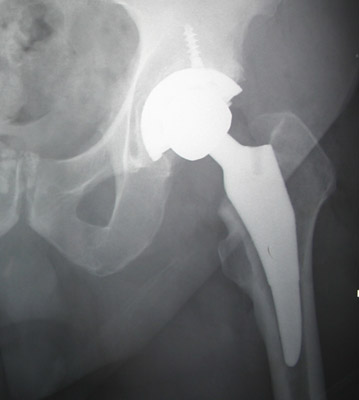
This is a short guide for my patients undergoing an Anterior Total Hip at the Scottsdale Joint Center. As Medical Director of the Scottsdale Healthcare Total Joint Center, I have now completed almost 1000 anterior total hip surgeries and have learned a few things to share with you about this procedure.

Compared to the last 1000 posterior hips I have done, the complication rate and recovery time is MUCH improved for the anterior hips. Our deep infection rate is .1 percent for the anterior hips, much less than the posterior hips. Our dislocation rate is .5% with anterior hips vs. 2.5% for posterior hips. Fracture rate is .2% for the anterior hips (minor fractures not requiring revision). Deep venous thrombosis ( clot in leg vein) rate is .1% for anterior hips vs. 1.5% for posterior hips. See the trend? In every category our complication rate is lower in the anterior hip group. Early mobility in the anterior hips allows us to avoid complications of extended bed rest.
Most patients preparing for a hip replacement want to know, “How fast can I return to work”? How fast can I return to tennis? When can I return to golf? When can I drive my car? What are my restrictions?

One of the many remarkable things about this procedure is that working patients can now “get their hip fixed”, without missing much work at all. I have now seen Many patients have the procedure on a Thursday morning, and be back in the office working on Monday! This is a game changer for many, as in the past patients had to delay their surgery, or plan to take a short term disability leave of absence. It is no longer necessary to do that if you have a “lighter duty” type job such as office work, or even light sales work. I have had realtors work and manage open houses a week after surgery. I believe I could return to my job as a physician in 4 or 5 days after an anterior hip (but I would book easier cases!)
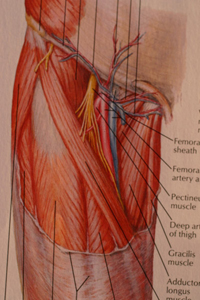
Not all anterior hip surgeons do the procedure the same way. I have embraced the minimally invasive aspects of this procedure that make it so special. Some surgeons will still take down some muscles to make the procedure easier to do, particularly in large muscular men. However, over time and through experience, I have perfected an operative approach that “almost never” has to do this. Therefore, I believe most of my patients recover as fast as possible. Other surgeons advertise the anterior hip, but do it without the special table. I do not believethey can do the job in the same minimally invasive fashion or have patients recover as fast as we do! I have had a number of patients go home the same day as surgery.

Recovery starts in the recovery room immediately after surgery. We minimize narcotic pain medicine whenever possible (because it is not needed, the procedure does not hurt like the posterior hips do!). Patients describe the pain to me as a muscle ache or “Charlie horse”, not a deep pain. We rate pain on a scale from 1 to 10, with 10 being the worst pain most people have experienced (often childbirth for women, and passing a kidney stone for men). Patients tell me their anterior hip pain is between 0 to 5.
(I don’t really understand the ZERO pain people either, but I am thankful for them!)
As soon as you get to the orthopedic floor ( where the nurses and therapists are specially trained to get you up right away), we think it is very important to avoid the narcotics that might make you nauseas or light headed, as it is crucial to get going out of bed. It is also so important to get the blood moving in your legs to avoid blood clots and stimulate healing! ( My results so far include 1 proximal DVT for 1000 anterior hips ( deep venous thrombosis), and I believe it is because we push you to get up right away! We get you up walking ASAP, as remarkably, patients tell me it hurts LESS to walk then laying in bed! It appears that most of the nerve endings are in the muscle attachments, and amazingly, cutting the bone only does not cause much pain.

Sometimes blood can collect in the wound, and it may cause pressure a day or two later, that is why we sometimes place a temporary drain tube in the hip to allow the fresh bleeding to come out ( we can also save your blood in a container that allows us to re-transfuse it back into you if you need it.) My rate of additional blood transfusion is very small, maybe one or two percent. That is why we no longer have you donate a unit of your own blood. It is rarely necessary. The drain is most often pulled by the nursing staff in the morning before discharge. Remarkably, Over ninety percent of my anterior hips are discharged on the day after surgery. The rest need to stay another day because of home related care issues, or because they are elderly or have a history of other medical risks. It has been most satisfying to see this rapid level of recovery. There is no other major orthopedic procedure quite like it in this regard. When you go home, you have virtually no activity restrictions. The anterior hips are remarkable resistant to dislocation. This is because the muscles that are not cut, span the joint and act like intact rubber bands under stretch to hold the hip in place.

The biggest distinction between anterior and posterior hips is the activity restrictions with posterior hips. Posterior hips dislocate a lot more! The posterior muscles that were cut to see the socket, no longer hold the hip in place if you flex up too far or cross your legs and “lever” the head out of the socket. Anterior hips can dislocate but it is a very rare occurrence (about .5%or 1/200 patients). So far in my personal series, the risk appears greater in significantly overweight women. This is due to differences in pelvis anatomy in men and women. A recent research paper shows why – Large thighs can push against each other during certain activities like getting up from a low soft chair. Their research model actually shows how one large thigh can push the other one out of joint during certain twisting maneuvers. We now add a little length to our women of this body type as that “tightens” the hip further by stretching the intact muscles even more (this results in holding the hip in place better – a slight leg length difference is well tolerated and well worth it for the extra protection it affords against dislocation!) We will talk about all these issues in the office before your surgery!

So back to recovery time. Remarkably, most patients are “done” about 6 weeks after surgery. Most are doing so well at 4 weeks, that they don’t fee l like they need to come back again to the office. . Lately, I have been telling patients to come back only if needed! (I will assume no news is good news! ) By the way, there is no formal physical therapy required after this anterior hip procedure! We give you home exercises to follow, and the hip rehabs itself quite well. This is a tremendous time saver and expense saver compared to the posterior hips. PT is used on the posterior hips because the cut muscles need to be rehabbed and the PT needs to emphasize the dislocation precautions!
You can swim as soon as the wound is healed (ten days). You can walk without support in a few days. Many patients use a cane for 10 days just for moral support and safety. You can drive your car in a few days, as long as you are off narcotics and feel safe controlling the vehicle. You can play golf around 3 weeks or so, and tennis about 6 weeks (although some have done it sooner). You can ride your horse safely in 30 days.

After that, progress as tolerated. We don’t recommend running sports (except doubles tennis), although many of my patients choose to do them. I will see how they do over time! Our restrictions are common sense based, after all the long term durability of the hip implants is unknown, and we would like them to last forever if possible! We use a new plastic that is MUCH stronger and more durable than anything we have used in the past, so we don’t know how long it will last. The manufacturer suggests the Vitamin E impregnated polyethylene will last 30+ years based on lab simulations of activity.
In short, this procedure is amazing. You should get through it without a major upheaval in your routine. As always, I must remind you that no surgery is guaranteed, and that complications can happen to anyone. But this procedure gives you your best odds of success if you need a hip replacement!